TL;DR:
- Skin fairness lacks a universal definition and varies across dermatology, AI, and social contexts, reflecting systemic biases. Current classification tools favor lighter skin tones, leading to clinical and technological disparities, with measurable AI biases corrected through targeted mitigation. Addressing these issues requires shifting toward objective, melanin-based systems and expanding societal efforts to promote inclusive, safe, and equitable skin standards worldwide.
Most people assume skin fairness is a simple, universal concept. It isn't. Defining skin fairness systems turns out to be one of the most contested areas across dermatology, artificial intelligence, public health, and social science. Each field applies different skin fairness criteria, uses distinct classification tools, and reaches different conclusions about what "fair" even means. Whether you're researching cosmetic products, skin-tone AI bias, or cultural beauty standards, understanding how these frameworks operate and where they break down gives you a much sharper view of a topic that affects billions of people.
Table of Contents
- Key takeaways
- Defining skin fairness systems: the dermatological foundation
- AI auditing and bias in skin tone systems
- Societal, behavioral, and regulatory dimensions
- Critiques and ethical considerations
- My perspective on where these systems fall short
- How skin fairness connects to digital skin design
- FAQ
Key takeaways
| Point | Details |
|---|---|
| No universal definition exists | Skin fairness criteria differ across dermatology, AI, cosmetics, and social science, with no single agreed standard. |
| Fitzpatrick types have real limits | The Fitzpatrick scale gives more categories to lighter skin, which structurally disadvantages darker skin tones in clinical and AI contexts. |
| AI fairness gaps are measurable | Frameworks like DermEquity found 0% sensitivity for the darkest skin category, with targeted mitigation reducing that bias gap by up to 68%. |
| Regulatory oversight matters | The FDA bans mercury in skin-lightening products and warns about hydroquinone due to documented health risks including permanent discoloration. |
| Ethical reform is overdue | Calls for more inclusive, pigment-informed classification systems are growing because current frameworks embed whiteness as the default standard. |
Defining skin fairness systems: the dermatological foundation
Before anything else, you need to understand that skin tone classification in medicine is not just a cosmetic exercise. These systems directly influence diagnosis, treatment decisions, and clinical outcomes. The most widely used framework is the Fitzpatrick Skin Type Scale, developed by dermatologist Thomas Fitzpatrick in 1975. It divides skin into six categories based on responses to UV exposure, ranging from Type I (very fair, always burns) to Type VI (deeply pigmented, never burns).
The scale gets used for everything from laser dosing to sunscreen recommendations to dermatological AI training data. However, it was originally designed to describe photosensitivity in lighter-skinned populations. That origin shows. The categories cluster more granularly around lighter skin tones, leaving darker complexions grouped broadly into just one or two types.
Other fair skin assessment techniques have emerged to address this gap:
- Individual Typology Angle (ITA): A spectrophotometric measurement of skin color using reflectance data, providing a numerical score rather than a categorical type.
- Monk Skin Tone Scale: Developed with Google AI, this 10-step scale was designed with more representation for darker skin tones.
- von Luschan scale: A historical chromatic scale using ceramic tiles for visual matching, now largely obsolete but historically significant.
- Melanin Index: A clinical measurement of melanin concentration using narrowband spectrophotometry.
| Classification System | Basis | Number of Categories | Key Limitation |
|---|---|---|---|
| Fitzpatrick Scale | UV photoreactivity | 6 | Biased toward lighter skin granularity |
| Monk Scale | Perceptual diversity | 10 | Newer, limited clinical validation |
| ITA | Spectrophotometric | Continuous | Requires specialized equipment |
| Melanin Index | Melanin concentration | Continuous | Not widely standardized |
Patients with darker skin also face distinct clinical challenges. Hyperpigmentation conditions, for example, require tailored approaches such as tinted mineral sunscreens that match the patient's skin tone, improving both adherence and psychosocial outcomes. These are not cosmetic preferences. They are clinical necessities that current classification systems often fail to accommodate well.

AI auditing and bias in skin tone systems
When machine learning tools entered dermatology, they brought existing classification biases with them. A model trained predominantly on lighter skin types will perform worse on darker skin types. This isn't speculation. It's measurable.
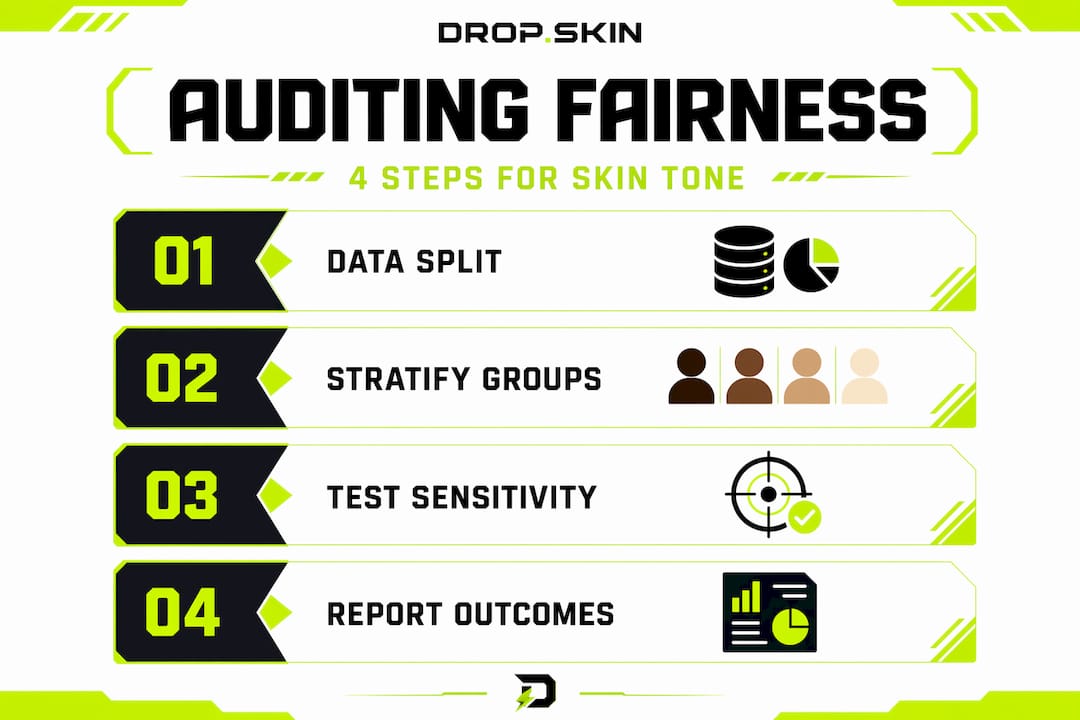
DermEquity is one of the most structured approaches to evaluating skin complexion systems in AI. It's an auditing toolkit that uses a defined workflow to detect and reduce bias in dermatological AI models. Here's how it works:
- Group definition: AI outputs are stratified by Fitzpatrick skin types to create measurable subgroups.
- Disparity measurement: Sensitivity, specificity, and accuracy are compared across these groups.
- Causal testing: Counterfactual skin-tone modifications are applied to images to isolate whether tone itself drives performance gaps.
- Mitigation selection: Techniques like synthetic LAB color space augmentation or balanced resampling are applied to reduce detected disparities.
The results from this approach are striking. DermEquity's auditing workflow found 0% sensitivity for the darkest skin category (Fitzpatrick Type VI) in some models, meaning the AI completely failed to detect conditions in the darkest skin tones. With targeted mitigation including synthetic LAB augmentation, bias gap reduction reached up to 68%. That's a significant improvement, but it highlights how serious the starting gap was.
The deeper problem is that counterfactual analysis reveals something the original category labels cannot: skin tone itself was causing the performance difference, not just underlying dataset imbalance. This distinction matters enormously for building fairer AI systems.
Pro Tip: When evaluating any AI-powered dermatological tool, ask vendors specifically about Fitzpatrick-stratified performance data. A tool that only reports aggregate accuracy is hiding the information you actually need to assess equity.
Skin fairness measurement methods in AI require more than a single accuracy number. They require auditable, group-stratified reporting across every major skin tone category. Anything less is an incomplete audit.
Societal, behavioral, and regulatory dimensions
The phrase "skin fairness" doesn't just live in clinics or AI labs. It lives in culture. And the social drivers behind skin-lightening practices are deeply documented and deeply complex.
Globally, demand for skin-lightening products is driven by a combination of social prestige attached to lighter skin, media representation, and, in many contexts, economic factors. Over 1 in 10 people in Jamaica report using skin-lightening products, which signals that this is a public health issue as much as a consumer behavior one. PAHO and WHO have both called for ingredient bans combined with surveillance and behavioral interventions.
The regulatory picture in the United States adds another layer. The FDA takes a specific, safety-focused stance on skin fairness criteria as they apply to products:
- Mercury: Banned due to toxicity in all skin-lightening products sold in the US.
- Hydroquinone: Flagged for causing rashes, facial swelling, and permanent skin discoloration. The FDA actively warns consumers against unsanctioned over-the-counter use.
- Steroid-based lighteners: Common in imported or counterfeit products, they carry risks of thinning skin and hormonal disruption.
"Safety must frame fairness systems that include skin lightening claims; unsafe ingredient use undermines true fairness by introducing health risks." — FDA consumer guidance
Social science adds yet another angle. Implicit bias research using skin-tone IAT (Implicit Association Tests) reveals that people associate lighter skin with positive attributes faster than they consciously report. This means that survey-based research alone undercounts the actual influence of skin tone bias on behavior. Any evaluating skin complexion system that relies only on self-reported preferences is structurally missing part of the picture.
Critiques and ethical considerations
The most uncomfortable truth about current skin fairness systems is that many of them were not designed with global skin diversity as the starting point. They were designed with lighter skin as the default, and darker tones were added in limited, underrepresented ways.
| System Type | Who it serves well | Where it falls short |
|---|---|---|
| Fitzpatrick Scale | Photosensitivity in lighter skin | Insufficient granularity for darker tones |
| "Skin of Color" (SOC) framing | US racial discourse | Not globally accurate for pigment diversity |
| AI diagnostic tools | Populations represented in training data | Performs poorly on darker skin types |
| Cosmetic "fairness" products | Consumer demand in certain markets | Reinforces colorism; safety risks |
The "skin of color" label deserves specific attention. It originated in US racial discourse and does not map cleanly onto global pigment diversity. Someone classified as "skin of color" in a US clinical context might be categorized entirely differently under a system designed in Brazil, South Africa, or India. These aren't just terminological quirks. They affect which conditions get studied, which products get developed, and which populations benefit from medical research.
The philosophical critique goes further. Classification systems that embed whiteness as the normative standard don't just fail scientifically. They actively reinforce social hierarchies through what looks like neutral technical language. Colorism, the preference for lighter skin within communities of color, is not separate from these systems. It's partially sustained by them.
Pro Tip: When reading clinical studies on skin conditions, check whether the study reports outcomes stratified by skin tone. If it doesn't, the findings may not apply evenly across skin types, regardless of how authoritative the source sounds.
Calls for pigment-informed dermatology frameworks that go beyond racial labels and use actual melanin measurement are gaining traction in academic dermatology. They represent one of the most promising paths toward truly inclusive skin fairness measurement methods. The skin's actual pigment content, measured objectively, is a more stable and equitable basis for classification than ancestry, self-identification, or subjective visual categories.
My perspective on where these systems fall short
I've spent a lot of time working at the intersection of classification systems and real-world outcomes, and what I keep seeing is the same mistake repeated across fields. People treat a classification system as if it's the territory rather than a map of the territory.
The Fitzpatrick scale is a useful tool. DermEquity is a useful tool. FDA guidance is necessary and important. But none of them, alone or together, constitutes a complete answer to what defines skin fairness. What I've found is that the most useful approaches are the ones that are honest about their own limitations.
The clinical community is slowly recognizing that treating hyperpigmentation as purely cosmetic misses the real patient burden. The AI community is recognizing that a single accuracy number masks serious inequities. The regulatory community is recognizing that banning mercury is necessary but not sufficient. These are real improvements, but they're incremental when the underlying category design problem remains unaddressed.
What I think needs to happen urgently is a shift from race-proxy classifications to melanin-based, objectively measured systems. Not because race doesn't matter socially. It absolutely does. But because using race as a proxy for skin tone in medical and technical contexts introduces exactly the kind of imprecision that fairness systems are supposed to eliminate.
The uncomfortable truth is that some of the systems we call "fair" are doing the opposite of what their name implies. Recognizing that is step one.
— Dropskin
How skin fairness connects to digital skin design
Understanding how skin tone classification works in the real world makes you a sharper thinker about fairness in digital spaces too. In gaming, skin patterns in CS2 follow their own kind of visual classification logic, where texture, finish, and color hierarchy determine perceived value. The principles are different, but the idea that classification shapes perception and value applies directly.
If you're interested in exploring how digital skin systems work in practice, Dropskin gives you a hands-on way to do it. At DROP.SKIN, you can open CS2 cases, upgrade skins, and experiment with customization in a platform built around community and transparency. The skin upgrader tool at DROP.SKIN's upgrader lets you trade up skins systematically, applying a logic not unlike the classification-to-value frameworks discussed in this article. For anyone curious about fairness in skin-based systems, the platform is a practical environment to see those principles in action.
FAQ
What is the Fitzpatrick scale used for?
The Fitzpatrick scale classifies skin into six types based on UV photoreactivity and is widely used in dermatology, laser treatment dosing, and AI training datasets. Its main limitation is that it provides more granular categories for lighter skin tones than for darker ones.
Why do AI skin tone systems show bias?
AI models trained on datasets that underrepresent darker skin tones consistently perform worse on those groups. DermEquity found 0% sensitivity for the darkest Fitzpatrick category in some models, a gap reducible by up to 68% with targeted mitigation techniques.
Are skin-lightening products safe to use?
The FDA warns that skin-lightening products containing mercury are banned in the US, and hydroquinone carries serious risks including permanent discoloration and facial swelling. Always check ingredient lists and consult a dermatologist before use.
What does "skin of color" mean in medical contexts?
The term originated in US racial discourse and refers broadly to non-white skin tones, but it lacks a universally accepted definition and does not accurately represent global pigment diversity. More precise, melanin-based frameworks are increasingly recommended by researchers.
How is implicit bias relevant to skin fairness systems?
Implicit Association Test research reveals that people unconsciously associate lighter skin with positive attributes faster than they report consciously. This means that self-report surveys undercount the true influence of skin tone bias, and robust fairness systems need to account for unconscious preference patterns.